The STEP 1 Trial: A Landmark in Obesity Medicine
The Semaglutide Treatment Effect in People with obesity (STEP) 1 trial stands as one of the most consequential clinical trials in the history of obesity medicine. Published in the New England Journal of Medicine in February 2021 by Wilding et al., this double-blind, randomized, placebo-controlled trial demonstrated that once-weekly subcutaneous semaglutide 2.4 mg produced unprecedented weight loss in adults with obesity or overweight [1].
Study Design and Population
STEP 1 enrolled 1,961 adults across 129 sites in 16 countries. Participants had a body mass index (BMI) of 30 or greater, or a BMI of 27 or greater with at least one weight-related comorbidity (hypertension, dyslipidemia, obstructive sleep apnea, or cardiovascular disease). Critically, participants did not have type 2 diabetes, distinguishing this trial from the SUSTAIN program that studied semaglutide for diabetes.
Participants were randomized 2:1 to receive either semaglutide 2.4 mg or placebo via once-weekly subcutaneous injection for 68 weeks, alongside lifestyle intervention consisting of counseling on diet (500 kcal/day deficit) and physical activity (150 minutes/week).
Primary Efficacy Results
The results exceeded expectations across all primary and secondary endpoints:
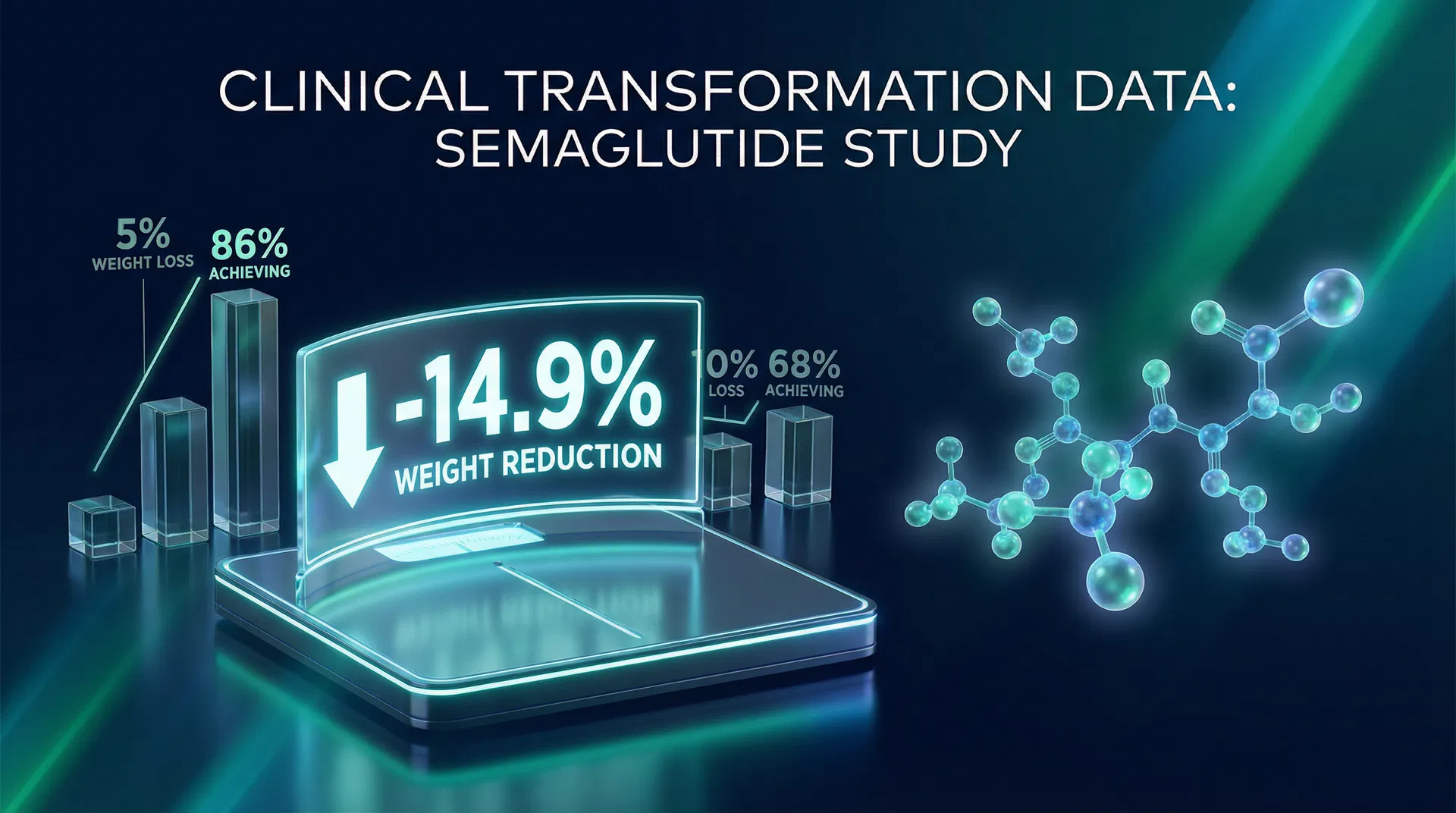
Mean Body Weight Change:
- Semaglutide group: -14.9% (approximately -15.3 kg)
- Placebo group: -2.4% (approximately -2.6 kg)
- Treatment difference: -12.4 percentage points (95% CI, -13.4 to -11.5; P<0.001)
Categorical Weight Loss Thresholds:
- ≥5% weight loss: 86.4% of semaglutide patients vs. 31.5% placebo
- ≥10% weight loss: 69.1% vs. 12.0%
- ≥15% weight loss: 50.5% vs. 4.9%
- ≥20% weight loss: 32.0% vs. 1.7%
These results meant that approximately one in three patients on semaglutide lost more than 20% of their body weight — a threshold previously achievable only through bariatric surgery [1].
Beyond the Scale: Cardiometabolic Improvements
STEP 1 demonstrated that semaglutide's benefits extended well beyond weight reduction:
- Waist circumference: -13.54 cm vs. -4.13 cm (difference: -9.42 cm)
- Systolic blood pressure: -6.16 mmHg vs. -1.06 mmHg
- C-reactive protein (CRP): -59.6% vs. -6.3%, indicating reduced systemic inflammation
- HbA1c: -0.45% vs. -0.15% (in non-diabetic participants)
- Fasting lipids: Significant improvements in triglycerides and VLDL cholesterol
Physical functioning scores, as measured by the SF-36 questionnaire, also improved significantly in the semaglutide group, suggesting meaningful quality-of-life benefits [1].
Safety Profile
The most common adverse events were gastrointestinal in nature, consistent with the GLP-1 receptor agonist class:
- Nausea: 44.2% semaglutide vs. 17.4% placebo
- Diarrhea: 31.5% vs. 15.7%
- Vomiting: 24.8% vs. 6.2%
- Constipation: 24.2% vs. 10.1%
Most gastrointestinal events were mild to moderate in severity and occurred primarily during the dose-escalation phase (weeks 1-16). Discontinuation due to adverse events occurred in 7.0% of the semaglutide group vs. 3.1% of the placebo group.
Serious adverse events occurred in 9.8% of semaglutide patients vs. 6.4% of placebo patients. Gallbladder-related disorders were more common with semaglutide (2.6% vs. 1.2%), consistent with rapid weight loss [1].
Subgroup Analyses
The weight loss benefit of semaglutide was consistent across prespecified subgroups, including:
- Age groups (18-40, 40-65, ≥65 years)
- Sex (male and female)
- Race and ethnicity
- Baseline BMI categories
- Geographic regions
This consistency strengthened the generalizability of the findings across diverse patient populations [2].
Impact on Clinical Practice
STEP 1 provided the pivotal efficacy data that supported the FDA's approval of semaglutide 2.4 mg (marketed as Wegovy) for chronic weight management in June 2021. The trial established several important precedents:
-
Pharmacotherapy can approach surgical outcomes: The ~15% mean weight loss and 32% of patients achieving ≥20% loss challenged the long-held view that only bariatric surgery could produce clinically meaningful weight reduction.
-
Obesity as a treatable chronic disease: The magnitude of benefit reinforced the concept that obesity is a chronic disease requiring ongoing medical treatment, not simply a lifestyle choice.
-
Setting the benchmark: STEP 1 became the standard against which all subsequent anti-obesity medications — including tirzepatide and retatrutide — would be compared.
Limitations
The trial had several important limitations. The 68-week duration, while substantial, did not address long-term outcomes beyond approximately 16 months. The study population excluded individuals with type 2 diabetes (addressed in STEP 2). Additionally, the trial did not assess what happens after treatment discontinuation (addressed in STEP 1 extension and STEP 4) [1].
References
-
Wilding JPH, Batterham RL, Calanna S, et al. "Once-Weekly Semaglutide in Adults with Overweight or Obesity." New England Journal of Medicine. 2021;384(11):989-1002. PubMed: 33567185
-
Bergmann NC, Davies MJ, Lingvay I, Knop FK. "Semaglutide for the treatment of overweight and obesity: A review." Diabetes, Obesity and Metabolism. 2023;25(1):18-35. PMC: 10092086
-
Kushner RF, Calanna S, Davies M, et al. "Semaglutide 2.4 mg for the Treatment of Obesity: Key Elements of the STEP Trials 1 to 5." Obesity. 2020;28(6):1050-1061. PubMed: 32441473